10 Leadership Styles in Nursing Explained
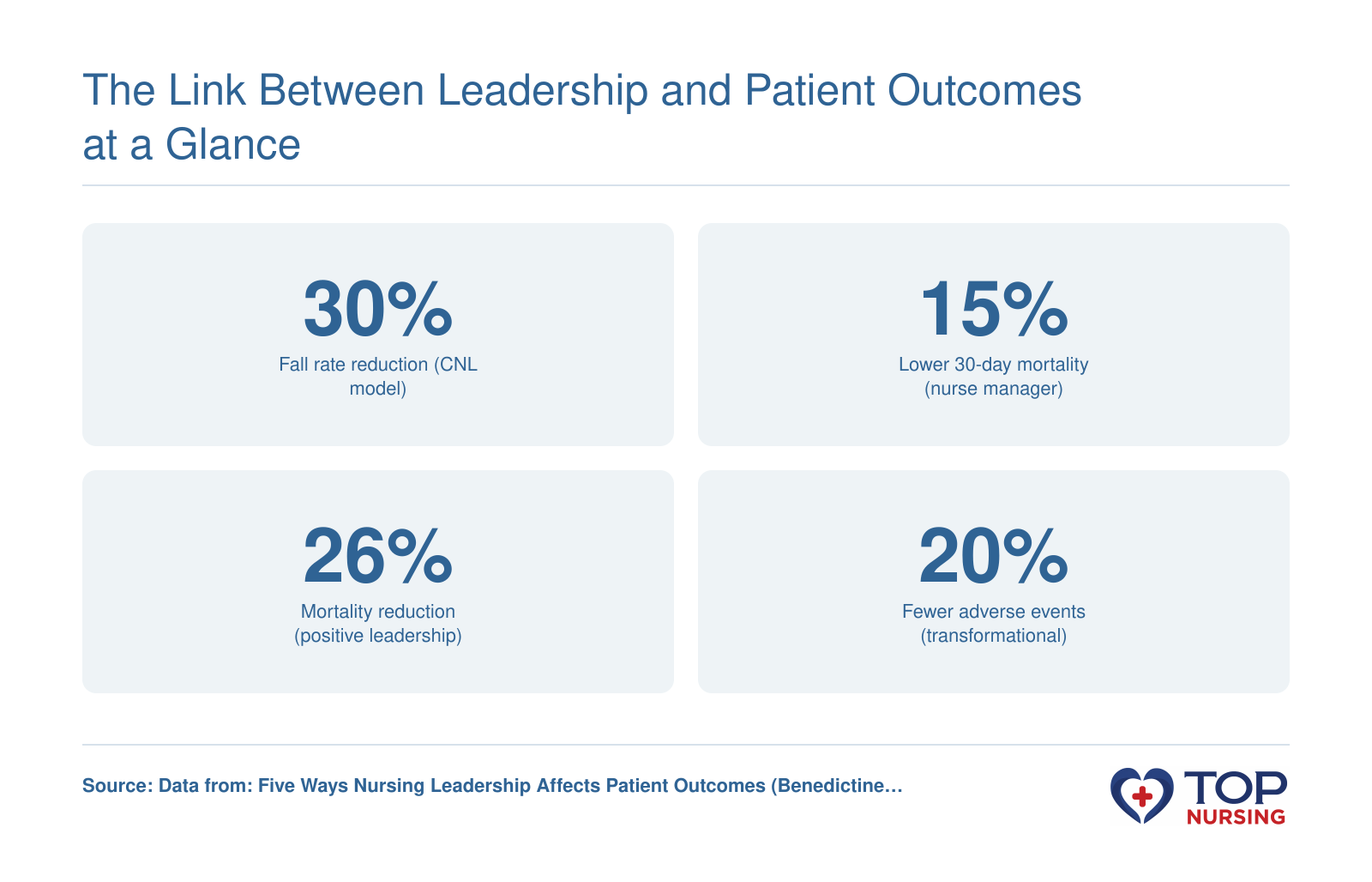
The leadership style you lean on most can either sharpen clinical decision-making or quietly erode team morale, and the difference shows up in patient outcomes. No single approach works in every unit, and the best nurse leaders learn to flex across several. Below, each style is broken down so you can spot when it helps, when it harms, and how it directly touches care quality.
Transformational Leadership
Transformational leaders inspire teams toward a shared vision by modeling enthusiasm and intellectual stimulation. They challenge the status quo and develop staff through mentorship. Key behaviors: articulating a compelling mission, encouraging innovation, and providing individualized support. Quality-impact callout: This style often raises patient satisfaction and reduces adverse events, but over-reliance can burn out staff who feel constant pressure to overperform.
Transactional Leadership
Built on clear exchanges of rewards for compliance and correction for errors, transactional leadership in nursing prioritizes structure and accountability. It thrives on defined roles and performance metrics. Key behaviors: setting explicit expectations, using contingent rewards, and monitoring deviations closely. Quality-impact callout: Highly effective for enforcing infection-control protocols and medication-safety checks, but when applied rigidly it stifles critical thinking and can miss early signs of patient deterioration that require initiative beyond the rulebook.
Democratic Leadership
Also called participative leadership, democratic leadership in nursing invites team input before decisions are made. Staff nurses feel heard and are more likely to commit to changes they helped shape. Key behaviors: facilitating open forums, soliciting bedside perspectives, and building consensus on unit improvements. Quality-impact callout: Improves care coordination and error reporting, yet it slows down crisis response: during a code blue, consensus-building can cost precious seconds.
Autocratic Leadership
Autocratic leadership in nursing places decision-making authority squarely on the leader, with little staff input. This style can appear during rapid emergencies when a single clear voice is needed. Key behaviors: issuing direct orders, centralizing control, and expecting immediate compliance. Quality-impact callout: Lifesaving in trauma or resuscitation, autocratic leadership prevents hesitation; however, chronic use breeds resentment, lowers morale, and suppresses the kind of frontline feedback that catches near-misses.
Laissez-Faire Leadership
Leaders adopting a laissez-faire style provide minimal direction and give experienced teams wide autonomy. It works only when staff are highly competent and self-motivated. Key behaviors: delegating broadly, avoiding micromanagement, and intervening only when asked. Quality-impact callout: Can foster innovation in seasoned ICU teams but frequently leads to role confusion, missed documentation, and fragmented care if staff lack the skills or initiative to self-regulate.
Servant Leadership
Servant leaders flip the hierarchy: their primary focus is serving the clinical team so nurses can serve patients better. This style emphasizes empathy, listening, and removing obstacles. Key behaviors: actively asking “What do you need to do your job safely?”, advocating for resources, and putting staff well-being above personal agenda. Quality-impact callout: Strongly linked to lower burnout and higher patient experience scores, but in a severely understaffed unit it may inadvertently delay hard decisions about performance accountability.
Visionary Leadership
Visionary leaders paint a vivid picture of a better future and rally the team around that destination. They excel during transitions: launching a new unit, implementing an EHR, or redesigning care models. Key behaviors: communicating purpose relentlessly, aligning small wins with the big picture, and maintaining a solutions-oriented tone. Quality-impact callout: Sparks engagement during change initiatives, but when the vision is disconnected from daily operational realities, staff grow cynical and basic care routines slip.
Bureaucratic Leadership
Bureaucratic leadership in nursing leans heavily on policies, procedures, and the chain of command. It ensures consistency and compliance with regulatory standards. Key behaviors: strictly adhering to clinical guidelines, documenting every step, and reinforcing established protocols. Quality-impact callout: Essential for accreditation readiness and high-risk areas like chemotherapy administration, it reduces variation in practice but can slow adaptation to a crashing patient or individual patient needs when the rulebook lacks an answer.
Situational Leadership
Situational leaders adjust their style (directive, coaching, supporting, or delegating) to match the competence and commitment of each nurse in each scenario. It’s a fluid, diagnostic approach. Key behaviors: assessing task readiness, flexing between supportive and directive behaviors, and providing just-right oversight. Quality-impact callout: Because it tailors supervision to the moment, situational leadership maximizes both safety with novices and autonomy with experts, but requires high emotional intelligence that can fatigue a leader during unrelenting shifts.
Authentic Leadership
Authentic leaders cultivate trust through transparency, self-awareness, and ethical consistency. They admit mistakes, share the reasoning behind tough calls, and stay relationally accessible. Key behaviors: aligning actions with stated values, seeking honest feedback, and modeling psychological safety. Quality-impact callout: Authentic leadership strengthens team cohesion and speaking-up behaviors that protect patients, yet when over-disclosure of leader uncertainty occurs during crises it can heighten staff anxiety and erode confidence in unit direction.
Overlaps with the NHS Healthcare Leadership Model
The NHS model describes seven core leadership styles: transformational, collaborative (closely aligned with democratic and servant styles), authoritative (similar to visionary and to aspects of autocratic leadership used judiciously), coaching (embedded in situational and authentic approaches), transactional, and command (pure autocratic). Bureaucratic leadership is not explicitly named but overlaps with elements of transactional and command styles focused on procedure. Recognizing these connections can help nurses moving between health systems adapt their language and expectations around leadership development.